
A new study of 20 of the world’s richest countries found it’s dangerous to be born into the United States.
The U.S. ranks last in child health outcomes compared to 19 other Organization for Economic Cooperation and Development nations with similar levels of economic development and political structures, including Australia, Canada, France, Sweden, Switzerland and the United Kingdom, according to the study published in Health Affairs, a peer-reviewed health care journal.
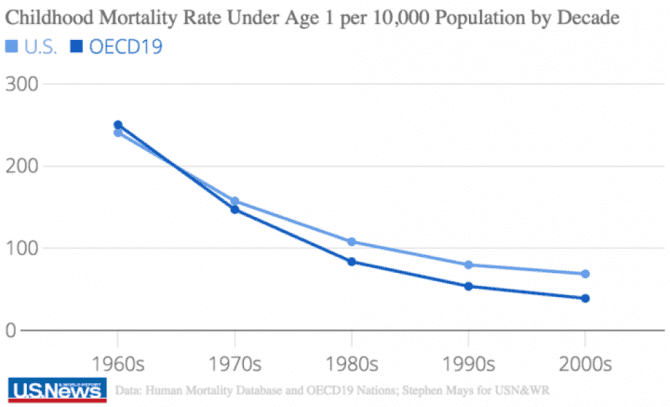
In fact, a child born in the U.S. is 76 percent more likely to die before their first birthday than infants born in other wealthy countries, and children who survive infancy have a 57 percent greater risk of death before reaching adulthood. The findings – based on a 50-year time-trend analysis from 1960 to 2010 – come despite America’s greater per capita spending on health care for children, the study notes.
“Every child should have the chance to live a full, healthy and safe life. This study shows that we are not living up to that promise and that we have fallen short of that promise for the last three decades,” says lead author Ashish Thakrar, an internal medicine resident at the Johns Hopkins Hospital. “Compared to these 19 similar countries, we are an outlier: This is the most dangerous of wealthy, democratic countries to be born into.”
The U.S. kept pace with child mortality rates in its peer nations in the 1960s, but researchers found that changed just a decade later. By the 1970s, U.S. mortality rates were noticeably higher for Americans ages 1 through 19 and by the 1980s, U.S. children under a year were also showing greater rates of mortality.
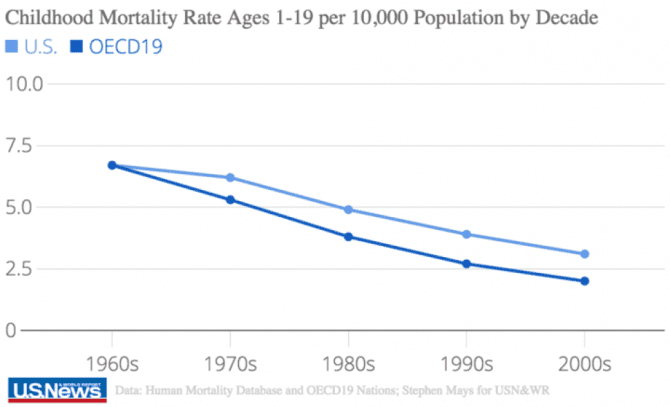
The shift was stark. Researchers say if the U.S. had achieved just the average childhood mortality rate of the other countries over the study period, more than 600,000 deaths could have been avoided.
In the U.S., Southern states hold some of the highest infant mortality rates, with Alabama, Mississippi, Oklahoma, Arkansas and Louisiana among the five worst states for infant mortality, according to 2017 U.S. News Best States data.
Thakrar and his team suggest America’s higher mortality rates are linked to its “persistently high poverty rates, poor educational outcomes, and a relatively weak social safety net.”
“There won’t be a quick fix for these disparities, but that is also no excuse for complacency,” Thakrar says.
The key takeaway from the study, Thakrar says, is that there are preventable deaths and that key players must think past medical care to address issues within American society. The U.S. does not have room to fall behind.
What’s more, the average life expectancy in the U.S. continued to drop for the second year in a row in 2016 as the ongoing opioid epidemic ravaged the nation – a trend that hadn’t been seen since the 1960s. And the U.S. has had one of the highest rates of child poverty among its wealthy counterparts since the 1980s.
The study’s authors suggest U.S. policy should strongly push reforms for infants that address deaths immediately before and after birth and for children between the ages of 15 and 19 related to automobile accidents and assaults by firearm. From 2001 to 2010, the study found, children ages 15 to 19 were 82 times more likely to die from gun homicide in the U.S.
The study contends that all U.S. policymakers, pediatric health professionals, child health advocates and families “should be troubled” by the findings.
“The care of children is a basic moral responsibility of our society,” the report says.
Even though the U.S. spends more on children’s health care per capita than the other nations, the authors’ unadorned conclusion was that the U.S. is “the most dangerous of wealthy nations for a child to be born into.”
One of the top five causes of infant deaths in the U.S. is sudden infant death syndrome (SIDS), which, by definition, is an unexpected and unexplainable death that occurs in a “seemingly normal, healthy infant under one year of age.” The Centers for Disease Control and Prevention (CDC) views SIDS (along with “accidental suffocation in a sleeping environment” and “other deaths from unknown causes”) as manifestations of the broader phenomenon of sudden unexpected infant death (SUID). CDC attributes three-fourths (75%) of the 3,700 annual SUID deaths (a conservative estimate) to SIDS and “unknown causes.”
The pronounced bifurcation that characterizes infant mortality in the U.S. versus the other 19 countries began in the 1980s. It would make sense to ask whether something happened at that time that could explain why American children began having a tougher time making it past their first birthday than children in Canada, Australia, New Zealand, Western Europe, Iceland or Japan, yet the Health Affairs authors propose only that differences in income, education and the social safety net are to blame.
There is no reason to believe that those factors dramatically worsened in the 1980s. However, there is another “elephant in the room” explanation that the Health Affairs authors studiously ignore: in the 1980s, there was a major uptick in vaccination, including a strong push to enact and enforce vaccine mandates in schools and, toward the close of the decade, a significant jump in the total number of vaccines required.
Without even counting the vaccines now routinely administered prenatally, American infants receive more vaccines in their first year than infants anywhere in the world and far more than in the 1980s. Many of those vaccines are administered in bundles at well-baby visits around two and four months—exactly when nine out of ten SIDS deaths occur.
Evidence of a SIDS-vaccine relationship
In 2017, the U.S. Court of Federal Claims ruled that there was “preponderant evidence” supporting a claim that vaccines “caused or substantially contributed” to a 2011 SIDS death. The court, which has a notoriously high burden of proof, also ruled that the death could not be attributed to non-vaccine-related factors.
A variety of epidemiologic and neuropathologic studies provide scientific context for the Court’s landmark SIDS determination. For example, a VAERS study by independent investigators scrutinized 1,881 reported infant deaths following receipt of one to eight vaccines and found that the deaths represented almost 5% of all adverse events reported for infants from 1990 through 2010. The authors then considered the childhood vaccine schedule over the 20-year period and determined that there was “a positive correlation between the number of vaccine doses administered and the percentage of…deaths” as well as hospitalizations. When the same authors also conducted a cross-national study to compare vaccine schedules and infant mortality rates across 34 countries, they reported “a high statistically significant correlation between increasing number of vaccine doses and increasing infant mortality rates.”
Case reports offer an even more concrete form of evidence linking vaccines to at least some SIDS fatalities. A study in Italy published in 2014 described histological examination of the autonomic nervous system in over 100 SIDS victims for whom detailed clinical and environmental information was available. After finding that 12% of the SIDS deaths occurred within one to seven days of the infant receiving a hexavalent vaccine for diphtheria, tetanus, acellular pertussis, Haemophilus influenzae type B, poliovirus and hepatitis B, the authors concluded that “vaccine components could have a direct role in sparking off a lethal outcome in vulnerable babies.” A case report from 2008, also by Italian researchers, described a three-month-old infant who died within 24 hours of receiving a hexavalent vaccine. Drawing on clinical data, postmortem findings and immunohistochemical and laboratory analyses, the investigators concluded that “acute respiratory failure likely due to post hexavalent immunization-related shock was the cause of death.”
“No concerning patterns?”
Unfortunately, researchers at the CDC and the U.S. Food and Drug Administration (FDA)—the two agencies charged with protecting children’s health and conducting vaccine surveillance through the Vaccine Adverse Event Reporting System (VAERS)—seem unconcerned about infant deaths that are temporally associated with vaccination. Three recent examples illustrate the agencies’ relaxed perspective:
- In a 2015 publication in Lancet Infectious Diseases, CDC and FDA researchers analyzed 783 deaths reported to VAERS from 2000 through 2012 following receipt of an individual or combination vaccine containing an inactivated poliovirus (IPV) component. The majority of reports involved children under age seven who received multiple simultaneous vaccines, and nearly all of the reported deaths (96%) were in children less than 12 months of age. For most (52%) of the deceased infants, SIDS was the reported cause of death. However, because the post-IPV SIDS reports “were consistent with reporting patterns for other vaccines,” the investigators found no cause for alarm.
- A CDC analysis in 2017 looked at over 20,000 VAERS reports (2005–2015) pertaining to hepatitis B-containing vaccines—administered to American babies from birth. The researchers found that half (51%) of all the adverse events reported for hepatitis B-containing vaccines were for children under two years of age, and SIDS was the most commonly reported cause of death. Nonetheless, the review “did not reveal new or unexpected safety concerns.”
- A third study by CDC researchers covering the time period from 1997 through 2013 characterized “main causes of death” among reports submitted to VAERS. Almost seven in ten deaths (68.4%) were in children, 57% of whom were male. Death certificates or autopsy reports, available for about 85% of child deaths, showed that SIDS was the top cause of death (44%), with asphyxia (6%) occupying second place. Although the CDC authors reported (for the child death reports) that “79.4% received >1 vaccine on the same day,” they noted “no concerning pattern.”
The two U.S. agencies and many of their international counterparts appear to be more interested in promoting across-the-board vaccination than in trying to find the cause of post-vaccination infant deaths. In numerous settings, officials take advantage of classification loopholes to mask the role of vaccines. In India, for example, a national committee charged with investigating 54 infant deaths that occurred following administration of an all-in-one pentavalent vaccine (similar to the hexavalent vaccine but without the polio component) sidestepped the possible role of the vaccine by rating 52 out of the 54 deaths as either coincidental or unclassifiable. In Vietnam, the World Health Organization (WHO) willingly reported a link between the pentavalent vaccine and non-fatal serious adverse events but termed all of the fatal cases in 12 previously healthy babies as not vaccine-related—despite reports that “hours after receiving the vaccine, they began wailing loudly, …had convulsions and serious trouble breathing [and] died shortly afterwards.”
The absence of a hard-and-fast definition of SIDS also contributes to the denialism about vaccines’ likely role. In the UK, researchers have described a growing reluctance among pathologists and coroners to even use the term SIDS, making assessment of SIDS data “potentially inaccurate and confusing.” In the U.S., non-standardized case definitions mean that “cases once reported as SIDS are now being reported as [accidental suffocation and strangulation in bed] and cause unknown/unspecified.” U.S. researchers also have shown that medical examiners and coroners are inconsistent in the cause of death that they apply to sudden unexpected infant deaths and often classify them as “suffocation/asphyxia.”
Inflammation and infection
Whether an infant death following vaccination eventually comes to be categorized as SIDS or something else, a common denominator in postmortem analyses is the ascertainment of “signs of inflammation and responses to infection” that are “out of proportion to preexisting symptoms.” The types of “mild problems” often listed as potential vaccine reactions are frequently observed in SIDS infants prior to death. Researchers have hypothesized that “the increase in inflammatory markers found in SIDS infants indicates that infection and inflammation might contribute to some of these deaths, either as a direct cause or the trigger of a lethal event” and “might also be indicative of vulnerability in the immune response to an infectious trigger in infants.” Vaccines—with their potent adjuvants designed expressly to stimulate an intense immune response—could well represent just such a trigger, with unfortunate consequences.