A method developed by Kary B. Mullis who won a Nobel Prize for its discovery. PCR was created to identify DNA viruses; the SARS-CoV2 virus, which has never been isolated, is allegedly an RNA virus. Therefore, multiple steps are necessary to “magnify” the amount of genetic material in the specimen. The PCR tests magnify DNA particles in a sample until they become visible. Journalist John O’Sullivan correctly warned that the massive PCR testing campaign could be a WHO vaccination program in disguise. Depending on how they are calibrated, they can pick up almost anything – even things that do not exist.
“PCR is a process that’s used to make a whole lot of something out of something. It allows you to take a very miniscule amount of anything and make it measurable and then talk about it like it’s important.” – Kary Mullis
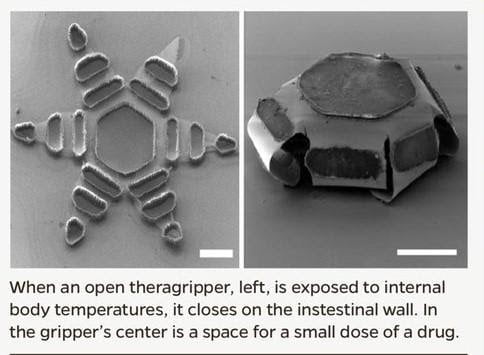
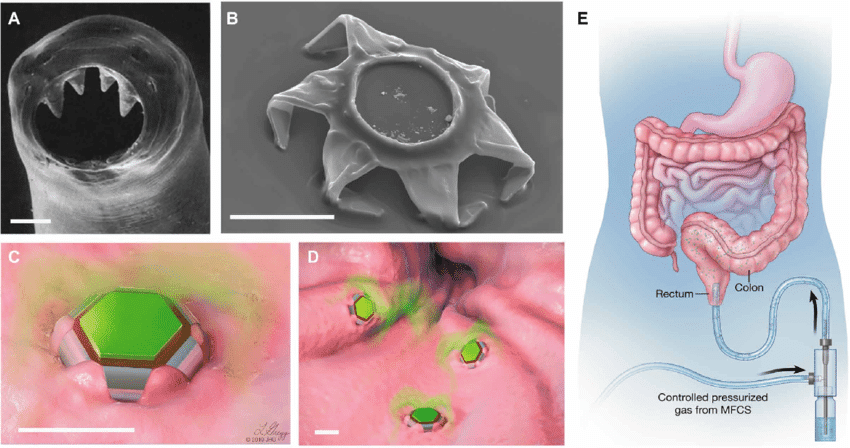
Johns Hopkins University developed tiny, star-shaped micro-devices called ‘Theragrippers’ that attach to the intestinal mucosa and that can deliver drugs into the body. The devices are made of metal and a thin film (a heat-sensitive kerosene wax) that changes shape and are as small as a dust particle. According to Johns Hopkins University, Theragrippers are administered with a cotton swab, similar to PCR tests. In October 2020, a Johns Hopkins University research team published positive results on Oct. 28, 2020 from an animal study confirming that the new technology works flawlessly.
Inspired by a parasitic worm that digs its sharp teeth into the intestines of its host, Johns Hopkins researchers have developed tiny, star-shaped micro-devices that attach to the intestinal mucosa and can deliver drugs into the body. (See Johns Hopkins University)

When the kerosene coating on the Theragripper reaches body temperature, the devices close autonomously and clamp onto the wall of the colon. Because of the sealing action, the tiny, six-pointed devices burrow into the mucosa and attach to the colon, where they are held and gradually release their drug load to the body. Eventually, the Theragripper lose their grip on the tissue and are removed from the colon through normal gastrointestinal muscle function.
Coincidentally, the PCR test in China is now also performed anally because the reliability of the results is said to be better and of course this practice is immediately supported in the Western mainstream media. (See Business Insider)
Note: If you can’t imagine the government administering toxins to you against your will and without your consent, think of all the horrific experiments on humans that were admitted afterwards and have continued well into modern times. In 2007, the CDC [8] even admitted that between 1955 and 1963, 10-30 million citizens were infected with the carcinogen SV40 via polio vaccination.
The “Test” doesn’t even test for Covid
“The magnification in PCR is measured by the number of cycles needed to make the DNA visible. Known as the Cycle Threshold (Ct) or Quantification Cycle (Cq) number, the higher the number of cycles the lower the amount of DNA in the sample,” explains the Brownstone Institute. “To convert Cq numbers into doses they have to be calibrated against the Cq numbers of standard doses. If they aren’t, they can easily be blown out of proportion and appear more significant than they actually are.”
An analogy for this might be a car advertisement in which the company used a scale model for the vehicle photo. After applying the right lenses, lighting and other touchups, that model is made to look like a full-size vehicle and consumers are none the wiser. The only way to truly know whether the vehicle in the photo is a small model or the real thing would be to put something else alongside it for a comparison of scale.
“Just like a coin standing next to a toy car proves it’s not a real one, and a shoe next to a molehill shows it’s not a mountain, the Cq of a standard dose next to the Cq of a sample shows how big the dose really is,” is how Brownstone puts it.
The method has never been validated properly as an instrument to detect disease – only detect fragments of the RNA of a virus (or Chromosome 8) – not a virus itself. This is important because COVID-19 has never been identified as an actual virus. And what makes this testing even more confusing is that the FDA admits that “The detection of viral RNA by RT-PCR does not necessarily equate with an infectious virus.”
Christian Drosten developed the fraudulent PCR Corona test in January 2020 (based on Dr. Kary Mullis’ PCR method), which from then on served as the standard method for detecting the Coronavirus SARS-CoV-2 worldwide. As Director of the Berlin Charité Institute, he is a very influential advisor to the German government and participated as an expert in many government press conferences. Thus, through his assessments, he also significantly influenced far-reaching political decisions, such as the compulsory wearing of masks, the suspension of regular school lessons, or the closure of the entire catering industry.
The Drosten-PCR-Tests, which were devised in January 2020, are not remotely suitable for determining whether someone is infected or not, despite being recommended as the global Gold Standard for determining infection by the WHO; it should be noted that the leadership of this organisation is under the financial control of China and the Bill & Melinda Gates Foundation (the WHO certainly has good employees – as too does the Robert-Koch Institute, despite its incompetent management).
In a retraction paper, a score of highly regarded international scientists have called on the editors of the journal which published the PCR tests as a measurement method for infections to withdraw the mischief forthwith. This test is not only scientific nonsense, but was obviously designed to create as many false positives as possible and so spread panic in the world. This English language retraction paper has been viewed about 18 million times. Furthermore, a second assertion made in January 2020 by Drosten that there are asymptomatic infections is false. These do not exist, as documented most recently by a major survey of ten million people from Wuhan of all places:
If a nasal or a blood sample contains a tiny snip of RNA from the SARS-CoV-2 virus, RT-PCR can possibly identify it. However – and this is important – a positive RT-PCR test result does not necessarily indicate a full virus is present. The virus must be fully intact to cross from person-to-person and cause illness. 90% of those who test positive using the PCR test, a method not meant to produce a positive or negative result, have such insignificant amounts of these RNA fragments that they are at no risk of illness and do not need to be quarantined.
Research published by the Spanish medical journal D-Salud-Discovery with a highly credible advisory board of eminently qualified physicians and scientists confirmed this. The genetic primers and probes used in RT-PCR tests to identify SARS-CoV-2 do not target anything specific. D-Salud-Discovery state there are no tests capable of identifying SARS-CoV-2. Consequently, all claims about the alleged impact of COVID 19 on population health are groundless. The entire official COVID 19 narrative is a deception. Ostensibly, there is no scientific foundation for any part of it.
The WHO’s Laboratory testing guidance states:
The etiologic agent [causation for the disease] responsible for the cluster of pneumonia cases in Wuhan has been identified as a novel betacoronavirus, (in the same family as SARS-CoV and MERS-CoV) via next generation sequencing (NGS) from cultured virus or directly from samples received from several pneumonia patients.”
The WHO’s claim is that the SARS-CoV-2 virus causes the disease COVID-19. They also allege this virus has been clearly identified by researchers in Wuhan.
In the WHO’s Novel Coronavirus 2019-nCov Situation Report 1, they state:
The Chinese authorities identified a new type of coronavirus, which was isolated on 7 January 2020……On 12 January 2020, China shared the genetic sequence of the novel coronavirus for countries to use in developing specific diagnostic kits.”
These two statements from the WHO clearly suggest the SARS-CoV-2 virus was isolated (meaning purified for study) and then genetic sequences were identified from the isolated sample. From this, diagnostic kits were developed and distributed globally to test for the virus in towns, cities and communities around the world. According to the WHO and Chinese researchers, these tests will find the virus that causes COVID 19.
Yet the WHO also state:
Working directly from sequence information, the team developed a series of genetic amplification (PCR) assays used by laboratories.”
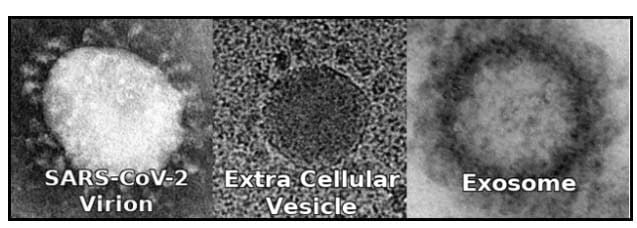
The Wuhan scientists developed their genetic amplification assays from “sequence information” because there was no isolated, purified sample of the so called SARS-CoV-2 virus. They also showed electron microscope images of the newly discovered virions (the spiky protein ball containing the viral RNA.)
However, such protein structures are not unique. They look just like other round vesicles, such as endocytic vesicles and exosomes.
Virologists claim that it is not possible to “isolate” a virus because they only replicate inside host cells. They add that Koch’s postulates do not apply because they relate to bacteria (which are living organisms). Instead, virologists observe the virus’ cytopathogenic effects (CPE), causing cell mutation and degradation, in cell cultures.
When Chinese researchers first sequenced the full SARS-CoV-2 genome they observed CPE in Vero E6 and Huh7 cells. Vero E6 are an immortalised monkey cell line and Huh7 are immortalised cancer (tumorigenic) cells. Meaning they have been maintained in vitro (in petri dish cultures) for many years.
Central to the official SARS-CoV-2 story is the idea that it is a zoonotic virus, capable of bridging the species gap from animals to humans. When scientists from the US CDC “infected” various cells with the novel virus they noted the following:
We examined the capacity of SARS-CoV-2 to infect and replicate in several common primate and human cell lines, including human adenocarcinoma cells (A549) [lung celles], human liver cells (HUH7.0), and human embryonic kidney cells (HEK-293T), in addition to Vero E6 and Vero CCL81 [monkey cells]…No cytopathic effect was observed in any of the cell lines except in Vero cells [monkey cells]…HUH7.0 and 293T cells showed only modest viral replication and A549 cells [human lung tissue cells] were incompatible with SARS-CoV-2 infection.”
The CDC did not observe any CPE in human cells. They saw no evidence that this alleged virus caused any human illness. Nor did this supposed human virus show any notable replication in human cells, suggesting human to human infection would be impossible.
Noting this problem, a team of Polish scientists introduced this sequenced “virus” to human epithethelium (airway) cells. They observed the effects on these HAE cultures for 5 days. They noted much greater replication than the CDC scientists but ultimately stated:
“We did not observe any release of the virus from the basolateral side of the HAE culture.”
Meaning they did not see any evidence of the supposed virions breaching the cell wall membrane. Again suggesting this so called virus isn’t infectious in human beings. It is not clear that SARS-CoV-2 is a human virus capable of causing illness. It may not even physically exist. Is it nothing more than a concept based upon predictive genetic sequences?
VOYAGE OF DISCOVERY
The Wuhan Center for Disease Control and Prevention and the Shanghai Public Health Clinical Centre published the first full SARS-CoV-2 genome (MN908947.1 ). This has been updated many times. However, MN908947.1 was the first genetic sequence describing the alleged COVID 19 etiologic agent (SARS-CoV-2).
All subsequent claims, tests, treatments, statistics, vaccine development and resultant policies are based upon this sequence. If the tests for this novel virus don’t identify anything capable of causing illness in human beings, the whole COVID 19 narrative is nothing but a charade.
The WUHAN researchers stated that they had effectively pieced the SARS-CoV-2 genetic sequence together by matching fragments found in samples with other, previously discovered, genetic sequences. From the gathered material they found an 87.1% match with SARS coronavirus (SARS-Cov). They used de novo assembly and targeted PCR and found 29,891-base-pair which shared a 79.6% sequence match to SARS-CoV.
They had to use de novo assembly because they had no priori knowledge of the correct sequence or order of those fragments. Quite simply, the WHO’s statement that Chinese researchers isolated the virus on the 7th January is false.
The Wuhan team used 40 rounds of RT-qPCR amplification to match fragments of cDNA (complimentary DNA constructed from sampled RNA fragments) with the published SARS coronavirus genome (SARS-CoV). Unfortunately it isn’t clear how accurate the original SARS-CoV genome is either.
Karen Kingston, a former Pfizer employee and a biotech analyst, joined Stew Peters to reveal how the PCR tests many are subjected to are hijacking your genetic code and transmitting the information back to China.
In 2003 a team of researchers from from Hong Kong studied 50 patients with severe acute respiratory syndrome (SARS). They took samples from 2 of these patients and developed a culture in fetal monkey liver cells.
They created 30 clones of the genetic material they found. Unable to find evidence of any other known virus, in just one of these cloned samples they found genetic sequences of “unknown origin.”
Examining these unknown RNA sequences they found 57% match to bovine coronavirus and murine hepatitis virus and deduced it was of the family Coronaviridae. Considering these sequences to suggest a newly discovered SARS-CoV virus (new discoveries being ambrosia for scientists), they designed RT-PCR primers to test for this novel virus. The researchers stated:
Primers for detecting the new virus were designed for RT-PCR detection of this human pneumonia-associated coronavirus genome in clinical samples. Of the 44 nasopharyngeal samples available from the 50 SARS patients, 22 had evidence of human pneumonia-associated coronavirus RNA.”
Half of the tested patients, who all had the same symptoms, tested positive for this new alleged virus. No one knows why the other half tested negative for this novel SARS-CoV virus. The question wasn’t asked.
This supposed virus had just a 57% sequence match to allegedly known coronavirus. The other 43% was just “there.” Sequenced data was produced and recorded as a new genome as GenBank Accession No. AY274119.
The Wuhan researchers subsequently found an 79.6% sequence match to AY274119 and therefore called it a novel strain of SARS-CoV (2019-nCoV – eventually renamed SARS-CoV-2). No one, at any stage of this process, had produced any isolated, purified sample of any virus. All they had were percentage sequence matches to other percentage sequence matches.
ISOLATE NOTHING
Scientists are very annoyed because they keep saying the virus has been isolated but no one believes them. This is because, as yet, no one has provided a single purified sample of the SARS-CoV-2 virus. What we have instead is a completed genome and, as we are about to discover, it isn’t particularly convincing.
Investigative journalists Torsten Engelbrecht and Konstantin Demeter asked some of the scientists who said they had images of SARS-C0V-2 virions to confirm these were images of an isolated, purified, virus. None of them could.
In Australia scientists from the Doherty Institute, announced that they had isolated the SARS-CoV-2 virus. When asked to clarify the scientists said:
“We have short (RNA) sequences from the diagnostic test that can be used in the diagnostic tests”
This explains why the Australian government state:
The reliability of COVID-19 tests is uncertain due to the limited evidence base…There is limited evidence available to assess the accuracy and clinical utility of available COVID-19 tests.”
In The UK, in July, a group of concerned academics wrote a letter to the UK Prime Minister Boris Johnson in which they asked him to:
Produce independently peer reviewed scientific evidence proving that the Covid-19 virus has been isolated.”
To date (mid-December 2020) they have not received a reply.
Similarly, UK researcher Andrew Johnson made a Freedom of Information Request to Public Health England (PHE). He asked them to provide him with their records describing the isolation of a SARS-COV-2 virus. To which they responded:
PHE can confirm it does not hold information in the way suggested by your request.”
Canadian researcher Christine Massey made a similar freedom of information request, asking the Canadian government the same. To which the Canadian government replied:
Having completed a thorough search, we regret to inform you that we were unable to locate any records responsive to your request.”
In the U.S. the Centre For Disease Control (CDC) RT-PCR Diagnostic Panel state:
…No quantified virus isolates of the 2019-nCoV are currently available……..Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms.”
Last updated on 13th July 2020, the CDC are yet to obtain any pure viral sample from any patient said to have the disease of COVID-19. They openly admit their tests don’t necessarily show if SARS-CoV-2 is either present or causes COVID 19.
We are told that none of this matters. That we are ignorant and just don’t understand virology. Therefore, we must accept pictures of things we know could be something else and genetic sequences (which could be anything else) as conclusive proof that this virus, and the disease it is supposed to cause, are real.
TESTING FOR NOTHING
The WHO, and every government, think tank, policy steering committee, government scientific advisor, supranational institutions and others who promote the official COVID 19 narrative, assert that SARS-CoV-2 causes COVID 19.
While no one has ever produced a sample of this supposed virus, the alleged SARS-CoV-2 genome has been published. It is in the public domain.
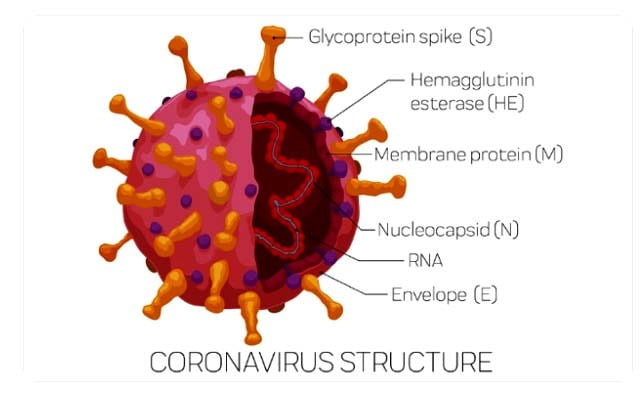
Key genetic sequences, in the SARS-CoV-2 genome, are said to have specific functions. These are the target proteins that scientists test for to identify the presence of the “virus”. These include:
- RNA-polymerase (Rd-Rp) gene – This enables the SARS-CoV-2 RNA to replicate inside the cytoplasm of COVID 19 diseased epithelial cells.
- S gene (Orf2) – this glycoprotein forms the spike on the SARS-CoV-2 virion surface which supposedly facilitates SARS-CoV-2 binding to the ACE2 receptors on cells, allowing the RNA inside the virion protein shell (capsid) to pass into the now infected cell.
- E gene (Orf1ab) – small membrane protein used in viral assembly
- N gene (Orf9a) – the nucleocapsid gene which binds the RNA in capsid formation
The WHO maintain a publicly available record of the RT-PCR primers and probes used to test for SARS-CoV-2. The primers are specific nucleotide sequences that bind (anneal) to the antisense and sense strands of the synthesized cDNA (called forward and reverse primers respectively.)
The cDNA strands separate when heated and reform when cooled. Prior to cooling, nucleotide sequences called probes are introduced to anneal to specific target regions of the suspected viral genome. During amplification, as the regions between primers elongate, when a primer strikes a probe, the probe decays releasing a fluorescent or dye which can then be read by researchers.
It is the identification of these markers which scientists claim to prove the presence of SARS-CoV-2 in a sample.
Something else which is publicly available is the Basic Local Alignment Search Tool (BLAST). This allows anyone to compare published nucleotide sequences with all those stored by the U.S. National Institutes of Health (NIH) genetic database called GenBank. Therefore we can BLAST the claimed SARS-CoV-2 primers, probes and target gene sequences.
The WHO’s forward, reverse primers and probe protocols, for the alleged SARS-CoV-2 viral genome, are based upon RdRp, Orf1, N and E gene profiles. Anyone can run them through BLAST to see what we find.
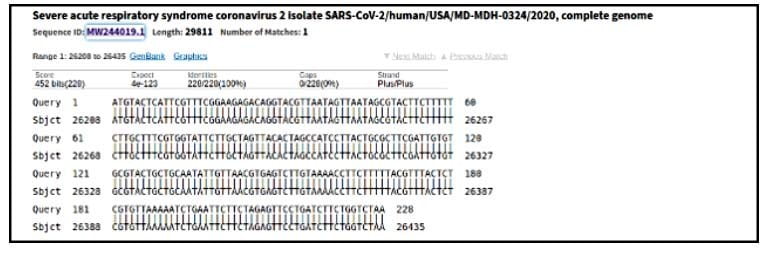
The vital RdRP nucleotide sequence, used as a forward primer is – ATGAGCTTAGTCCTGTTG. If we run a nucleotide BLAST this is recorded as a complete SARS-CoV-2 isolate with a 100% matched sequence identity. Similarly the reverse E gene primer sequence – ATATTGCAGCAGTACGCACACA – reveals the presence of the Orf1ab sequence which also identifies SARS-CoV-2.
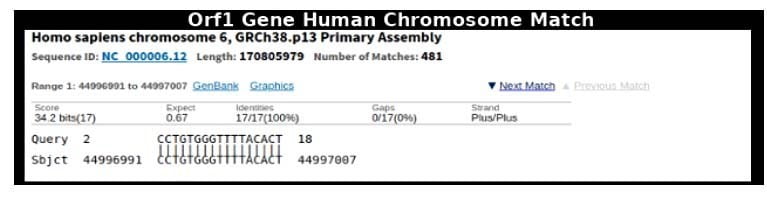
However, BLAST also enables us to search the nucleotide sequences of the microbial and human genomes. If we search for the RdRp SARS-CoV-2 sequence it reveals 99 human chromosome with a 100% sequence identity match. The Orf1ab (E gene) returns 90 with a 100% sequence identity match to human chromosomes.
Doing the same for these sequences with a microbial search finds 92 microbes with a 100% match to the SARS-CoV-2 E gene and 100 matched microbes, with a 100% sequence identity, to the vital SARS-CoV-2 RdRp gene.
Whenever we check the so-called unique genetic markers for SARS-CoV-2, recorded in the WHO protocols, we find complete or high percentage matches with various fragments of the human genome. This suggests that the genetic sequences, which are supposed to identify SARS-CoV-2, are not unique. They could be anything from microbial sequences to fragments of human chromosomes.
So called fact checkers, like Reuters’ Health Feedback project, have been quick to dismiss the claims of those who have noticed the apparent lack of specificity in the supposed SARS-CoV-2 genome.
Using a slew of strawman arguments like, “this claim suggests every test should be positive,” (which it doesn’t) their debunking attempt runs something like this:
Primers are designed to bind to specific nucleotide sequences that are unique to the virus. The forward primer may bind to a particular chromosome but the reverse primer doesn’t bind to the same chromosome and so the chromosome is not present in the SARS-CoV-2 virus. Moreover because the forward and perverse primers envelop the sequence to be amplified the cDMA sequence between primers is unique to the virus.
This seems to deliberately misrepresent the significance of these findings by forwarding an argument that no one, other than the fact checkers themselves, are making. BLAST searches show that these target sequences are not unique to SARS-CoV-2. Nor do all targets need to be found for a result to be deemed positive.
Moroccan researchers investigated the epidemiology of Moroccan alleged cases of SARS-CoV-2. Nine percent were positive for three genes, eighteen percent were positive for two genes and seventy three percent for just one. As we have just discussed, many may have been positive for none.
This is entirely in keeping with WHO’s test guidelines. They state:
“An optimal diagnosis consists of a NAAT [nucleic acid amplification test] with at least two genome-independent targets of the SARS-CoV-2; however, in areas where transmission is widespread, a simple single-target algorithm can be used……One or more negative results do not necessarily rule out the SARS-CoV-2 infection.”
Regardless of the spurious arguments of well funded fact checkers, if the forward and reverse primers identify junk, perhaps one being the fragment of a chromosome and the other a microbial sequence, then the amplified region between them is probably junk too.
The argument that RT-PCR only finds RNA is specious. Natural transcription (the separation of DNA strands) occurs during gene expression. No one is saying whole chromosomes or microbes are sequenced in the alleged SARS-CoV-2 genome. Though they may, for all we know. They are saying the alleged markers, used to test for this supposed virus, are not fit for purpose.
RT-PCR tests do not sequence the entire genome. They look for incidents of specific probe florescence to indicate the presence of sequences said to exist. These sequences are defined by MN908947.1 and the subsequent updates. These primers and probes could reveal nothing but RNA matches extracted from non-coding, sometimes called “junk,” DNA (cDNA.)
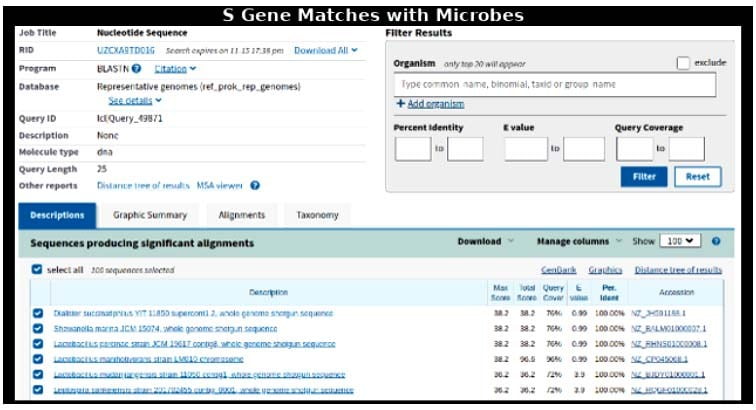
For example the SARS-CoV-2 S gene is meant to be highly specific to the SARS-CoV-2 virus genome. The target sequence is – TTGGCAAAATTCAAGACTCACTTTC. A microbial BLAST search returns 97 microbial matches with 100% identity sequence match. The lowest identity percentage match, within the top 100, is 95%. A human genome BLAST also finds a 100% sequence match to 86 human chromosome fragments.
No matter where you look in the supposed genome of SARS-CoV-2, there is nothing in the WHO’s test protocols that clearly identifies what it is. The whole genome could be false. The tests do not prove the existence of SARS-CoV-2. All they reveal is a soup of unspecified genetic material.
If so, as there are no isolates or purified samples of the virus, without a viable test, there is no evidence that SARS-CoV-2 exists. Therefore, nor is there any evidence that a disease called COVID 19 exists.
This infers that there is no scientific basis for any claims about COVID 19 case numbers, hospital admissions or mortality figures. All measures taken to combat this deadly virus are quite possibly founded upon nothing.
During Covid-19, authorities claim that testing is important for public health officials to assess if their mitigation efforts – “shelter in place” and “social distancing” and “wearing a mask” – are making a difference to “flatten the curve.” Officials also claim that testing is necessary to know how many persons have an infection within a community and to understand the nature of how coronaviruses spread.
Despite the challenges with test kits, testing began. By the end of March 2020, more than 1 million people had been tested across the US. By May 9, the number tested had grown to over 8.7M. Testing methods include a swab of the nasal passages or by inserting a long, uncomfortable swab through the nose to scrape the back of the throat. Specimens have also been obtained bronchoalveolar lavage, from sputum, and from stool specimens.
In February 2022, the CDC casually admitted some of the Covid nose swabs ended up in a lab for genomic sequencing analysis.
More on the swab below from Cassandra Dunn, RN and certified Federal Medical investigator, who documents the China-made nasal swabs are doused with highly toxic ethylene oxide which is mutigenic and harmful to ones health including lung diseases, cancer, and many other terrible health effects according to the EPA and FDA.
Repeat testing of persons who have a negative test may (eventually) confirm the presence of viral RNA, but this is impractical. Additionally, repeated testing of the same person can lead to even more confusing results. The test may go from negative, to positive, then back to negative again as the immune system clears out the coronavirus infection and moves to recovery.
From the Inventor of the test who says the method was never meant to be used as a test for a virus, Kary Mullis
“Scientists are doing an awful lot of damage to the world in the name of helping it. I don’t mind attacking my own fraternity because I am ashamed of it.”
From “CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel” [1]:
“Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms.”
Translation: A positive test doesn’t guarantee that the COVID virus is causing infection at all. And, ahem, reading between the lines, maybe the COVID virus might not be in the patient’s body at all, either.
From the World Health Organization (WHO): “Coronavirus disease (COVID-19) technical guidance: Laboratory testing for 2019-nCoV in humans” [2]:
“Several assays that detect the 2019-nCoV have been and are currently under development, both in-house and commercially. Some assays may detect only the novel virus [COVID] and some may also detect other strains (e.g. SARS-CoV) that are genetically similar.”
Translation: Some PCR tests register positive for types of coronavirus that have nothing to do with COVID—including plain old coronas that cause nothing more than a cold.
The WHO document adds this little piece:
“Protocol use limitations: Optional clinical specimens for testing has [have] not yet been validated.”
Translation: We’re not sure which tissue samples to take from the patient, in order for the test to have any validity.
From the FDA:
“LabCorp COVID-19RT-PCR test EUA Summary: ACCELERATED EMERGENCY USE AUTHORIZATION (EUA) SUMMARYCOVID-19 RT-PCR TEST (LABORATORY CORPORATION OF AMERICA)” [3]:
“…The SARS-CoV-2RNA [COVID virus] is generally detectable in respiratory specimens during the acute phase of infection. Positive results are indicative of the presence of SARS-CoV-2 RNA; clinical correlation with patient history and other diagnostic information is necessary to determine patient infection status…THE AGENT DETECTED MAY NOT BE THE DEFINITE CAUSE OF DISEASE (CAPS are mine). Laboratories within the United States and its territories are required to report all positive results to the appropriate public health authorities.”
Translation: On the one hand, we claim the test can “generally” detect the presence of the COVID virus in a patient. But we admit that “the agent detected” on the test, by which we mean COVID virus, “may not be the definite cause of disease.” We also admit that, unless the patient has an acute infection, we can’t find COVID. Therefore, the idea of “asymptomatic patients” confirmed by the test is nonsense. And even though a positive test for COVID may not indicate the actual cause of disease, all positive tests must be reported—and they will be counted as “COVID cases.” Regardless.
From a manufacturer of PCR test kit elements, Creative Diagnostics, “SARS-CoV-2 Coronavirus Multiplex RT-qPCR Kit” [4]:
“Regulatory status: For research use only, not for use in diagnostic procedures.”
Translation: Don’t use the test result alone to diagnose infection or disease. Oops.
“non-specific interference of Influenza A Virus (H1N1), Influenza B Virus (Yamagata), Respiratory Syncytial Virus (type B), Respiratory Adenovirus (type 3, type 7), Parainfluenza Virus (type 2), Mycoplasma Pneumoniae, Chlamydia Pneumoniae, etc.”
Translation: Although this company states the test can detect COVID, it also states the test can read FALSELY positive if the patient has one of a number of other irrelevant viruses in his body. What is the test proving, then? Who knows? Flip a coin.
“Application Qualitative”
Translation: This clearly means the test is not suited to detect how much virus is in the patient’s body. I’ll cover how important this admission is in a minute.
“The detection result of this product is only for clinical reference, and it should not be used as the only evidence for clinical diagnosis and treatment. The clinical management of patients should be considered in combination with their symptoms/signs, history, other laboratory tests and treatment responses. The detection results should not be directly used as the evidence for clinical diagnosis, and are only for the reference of clinicians.”
Translation: Don’t use the test as the exclusive basis for diagnosing a person with COVID. And yet, this is exactly what health authorities are doing all over the world. All positive tests must be reported to government agencies, and they are counted as COVID cases.
Those quotes, from official government and testing sources, torpedo the whole “scientific” basis of the test.
In an excellent interview with Celia Farber, she exposes many of the flaws in the test:
How many of us are “infected” with this novel Corona virus, and how scared should we be?
People die—yes. But people don’t die at the mercy of malicious, predatory pathogens, “lurking” on every surface, and especially other humans. That’s not “science.” That’s social engineering. Terrorism.
What do we mean when we say a person “tests positive” for Covid-19?
We don’t actually mean they have been found to “have” it. We’ve been hijacked by our technologies, but left illiterate about what they actually mean. In this regard, I spent time with, and interviewed the inventor of the method used in the presently available Covid-19 tests, which is called RT-PCR, (Polymerase Chain Reaction.). His name is Kary B. Mullis, he passed away in August of last year (2019). He was one of the warmest, funniest, most eclectic-minded people I ever met, in addition to being a staunch critic of HIV “science,” and an unlikely Nobel Laureate, i.e. a “genius.”
One time, in 1994, when I called to talk to him about how PCR was being weaponized to “prove,” almost a decade after it was asserted, that HIV caused AIDS, he actually came to tears. The people who have taken all of your freedoms away, they’re social engineers, politicians, globalist thought leaders, bankers, foundations, HO fanatics, and the like. Their army is composed of “mainstream media,” which is now literally a round-the-clock perfect propaganda machine in support of the so-called “Pandemic”.
Kary Mullis was a scientist. He never spoke like a globalist, and said once, memorably, when accused of making statements about HIV that could endanger lives: “I’m a scientist. I’m not a lifeguard.” That’s a very important line in the sand. Somebody who goes around claiming they are “saving lives,” is a very dangerous animal, and you should run in the opposite direction when you encounter them. Their weapon is fear, and their favorite word is “could.” They entrap you with a form of bio-debt, creating simulations of every imaginable thing that “could” happen, yet hasn’t.
Bill Gates has been waiting a long time for a virus with this much, as he put it, “pandemic potential.” But Gates has a problem, and it’s called PCR.
What does HIV have to do with Covid-19?
PCR played a central role in the HIV war (a war you don’t know about, that lasted 22 years, between Globalist post-modern HIV scientists and classical scientists.) The latter lost the war. Unless you count being correct as winning. The relentless violence finally silenced the opposition, and it seemed nobody would ever learn who these scientists were, or why they fought this thing so adamantly and passionately.
And PCR, though its inventor died last year, and isn’t here to address it, plays a central role in Corona terrorism.
Continue on next page…