

a failed nucleotide analogue RNA polymerase inhibitor drug developed in 2009 by Gilead Sciences to treat hepatitis C and respiratory syncytial virus (RSV), but it didn’t work against those diseases. In a failed attempt, they “repurposed” it for Ebola and Marburg viruses in 2014. It remained an unapproved drug due to failed trials (had the highest death rate of any test drug for Ebola and up to 74% side effects), yet it was not only authorized by the FDA for emergency use treatment of COVID-19 by Anthony Fauci and the NIH, it was THEE protocol drug for hospitals to follow, followed by the deadly ventilators.
Incidentally, remdesivir, the only drug ever approved for COVID, was developed by Dr. Ralph Baric’s lab at UNC Chapel Hill, the same lab that applied for the coronavirus spike protein gain-of-function research and is suspected by many to be behind the creation of this virus.
It was approved for emergency use by the FDA on May 1, 2020, and was subsequently fully approved by the FDA to treat ‘Covid-19’ on October 22, 2020. On January 22, 2022, the FDA granted expedited approval of a new supplemental drug application for Remdesivir, based on the recommendation of Fauci and the NIH.
Dr. Bryan Ardis made an astounding revelation stating that Dr. Fauci pushed the use of remdesivir as a treatment for COVID-19 knowing that it would be unsafe and ineffective for patients. Dr. Ardis revealed that the symptoms of lungs filling with fluid and the other alleged COVID-19 symptoms were actually side effects of kidney poisoning and other organ damage that are known side-effects of remdesivir. Dr. Ardis alleges that the devastating health toll allegedly caused by COVID-19 was actually caused by the NIH recommended treatment of remdesivir.
Dr. Bryan states that the NIH even cited two studies on its website that showed that remdesivir was ineffective and unsafe to patients. It seems that many doctors just blindly followed the recommendation of the NIH to use remdesivir without actually reading the cited studies. I tracked down those studies and read them.
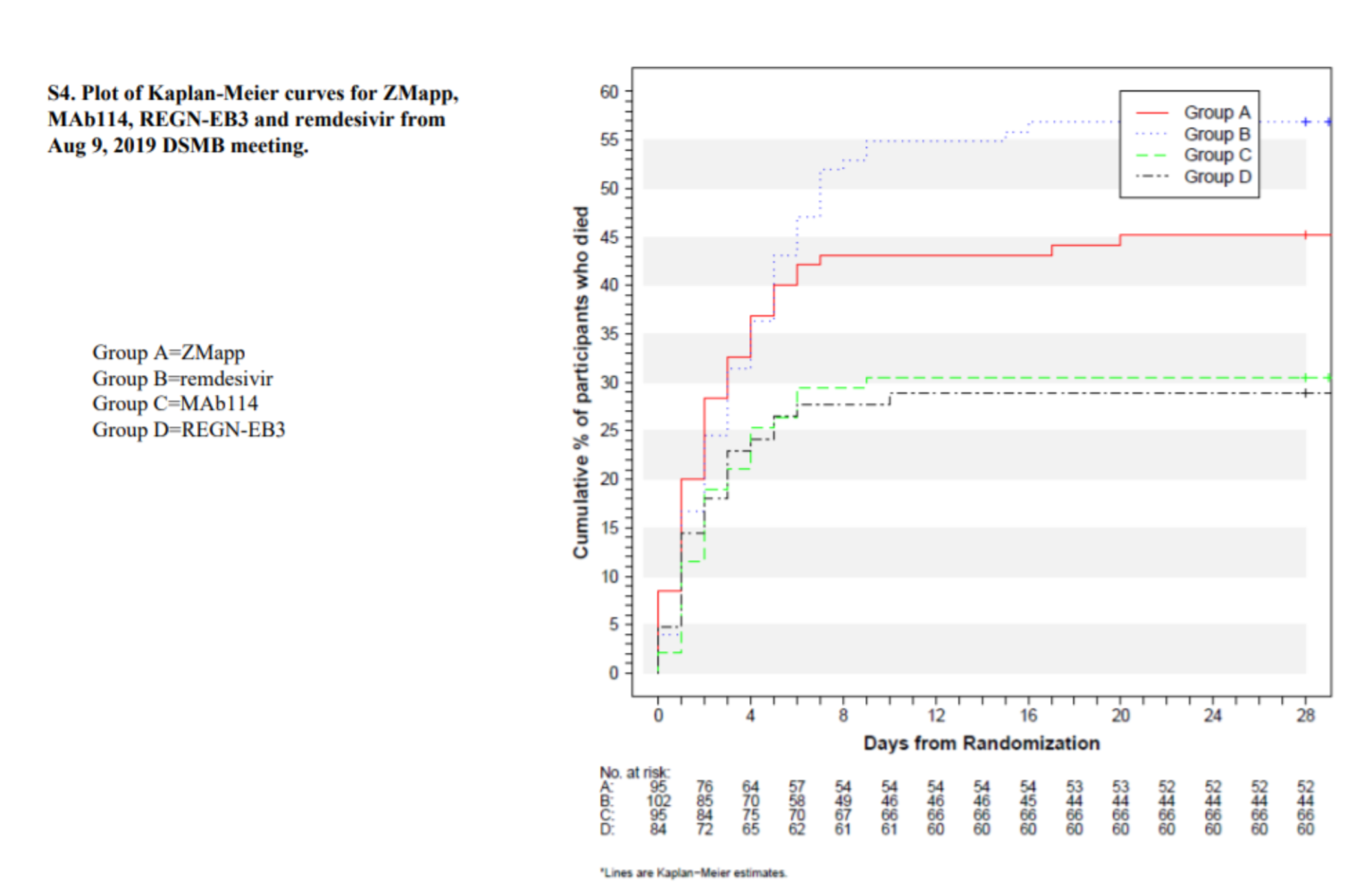
The New England Journal of Medicine published a study on remdesivir use in Ebola. Of the four drugs, remdesivir had the worst outcome with a 53.1% death rate, which is higher than the death rate from the virus. In fact, both remdesivir and ZMapp (death rate of 49.7%) were deemed to be so dangerous that they were pulled from the study on Aug. 9, 2019. Incidentally, Regeneron, which had the lowest death rate, is the monoclonal antibody therapy that seems to work well for COVID. Why would Fauci first pick remdesivir over Regeneron?
In another interview with Dr. Peter Breggin, Dr. Ardis said, “Anthony Fauci used this drug to mass murder a whole bunch of innocent Americans. Then he told you as he went on TV every night that people were dying in droves from a virus, when in fact the majority of them were being poisoned to death with remdesivir.”
Dr. Paul Marik, Founder of the FLCCC, testified about the dangers of remdesivir and the corruption in our medical system for prescribing it. Though it is deadly, doctors are being incentivized to use it on patients. Remdesivir killed more than 50% of the animals during its clinical trials. Yet the FDA still approved it.
Yet, in January and February of 2021 the NIH, in the ACTT 1 Study, enrolled patients in a study looking at Remdesivir for the treatment of Covid-19. The last patient was enrolled April 19, 2020. Ten days later, before the study had actually terminated, Dr. Fauci sat in the Oval Office of the White House and he said, “The trial was good news.”
What Dr. Fauci did not tell you was that the primary endpoint of the study was changed half-way during the study. We all know, that is scientific misconduct. Because the study was not going to be positive, they changed the primary endpoint.
The original endpoint was an 8-point scale that included death and a requirement for mechanical ventilation. Knowing that Remdesivir would not affect those endpoints, they invented a bogus endpoint called, “Time to Recovery.” Which they showed, in this study, was statistically significant. And based on this bogus endpoint, Remdesivir was approved by the FDA on October 20th, 2020.
So, if one does a meta-analysis looking at the studies of Remdesivir, the two studies, which were sponsored by Gilead, show a reduction in mortality. However, if you look at the four independent studies, including the large study by the WHO, it shows the opposite effect. Remdesivir increases the risk of death. Let me say that again. Remdesivir increases the risk of death by 3%. It increases your chance of Renal Failure by 20%. This is a toxic drug.
But, just to make the situation even more preposterous, the Federal Government will give hospitals a 20% bonus on the entire bill, if they prescribe Remdesivir to Medicare Patients. The Federal Government is incentivizing hospitals to prescribe a medication which is toxic.
So, it should be noted that Remdesivir costs about $3,000 a course. Dr. Kory spoke about Ivermectin. Ivermectin reduces the risk of death by about 50%. It costs the WHO two cents. Two cents.
So as regards dexamethasone, this is the wrong drug, in the wrong dose, for the wrong duration of time. Yet, every clinician in this country will absurdly use this homeopathic dose of dexamethasone. Why?! Because the N I H tells them to do this.
So, what the NIH and other agencies have ignored are multiple FDA approved drugs. These are FDA approved drugs. These are not experimental drugs, which are cost-effective, and safe, and have unequivocally been shown to reduce the death of patients in ICU and in hospital.
For example, there are 25 high quality studies (some people complain about the quality of these studies – so if you select out the high quality, randomized controlled trials) they show that Ivermectin reduces the risk of death by 26%. This is an extremely safe and cheap drug. In fact, it is one of the safest drugs on this planet. You are more likely to die from taking Tylenol…..
The recommendation from the NIH to use Veklury® (remdesivir) to treat COVID-19 came from the NIH Panel on COVID-19 Treatment Guidelines. There were nine (9) people on the NIH Panel on COVID-19 Treatment Guidelines with financial ties to Gilead Sciences, the maker of Veklury® (remdesivir).
The following is a list of those people on the NIH Panel on COVID-19 Treatment Guidelines who had financial ties to Gilead Sciences, the manufacturer of remdesivir:
- Rajesh Gandhi is on the advisory board of Gilead Sciences.
- David Glidden is a consultant for Gilead Sciences.
- Adaora Adimora is a consultant for Gilead Sciences and received research support from Gilead Sciences.
- Eric Daar is a consultant for Gilead Sciences and recieves research support from Gilead Sciences.
- Judith Aberg received research support from Gilead Sciences.
- Jason Baker received research support from Gilead Sciences.
- Susanna Naggie received research support from Gilead Sciences.
- Pablo Tebas received research support from Gilead Sciences.
- Roger Bedimo received an honoraria from Gilead Sciences.
Studies & Trials
Many of the studies cited in support of NIH’s recommendation to use Veklury® (remdesivir) were in vitro studies or animal studies. A couple of the human studies were at best a mixed bag. Two of the most authoritative studies showed Veklury® (remdesivir) to be ineffective and unsafe.
On or about May 12, 2020, the FDA reported the following summary for study GS-US-5773:
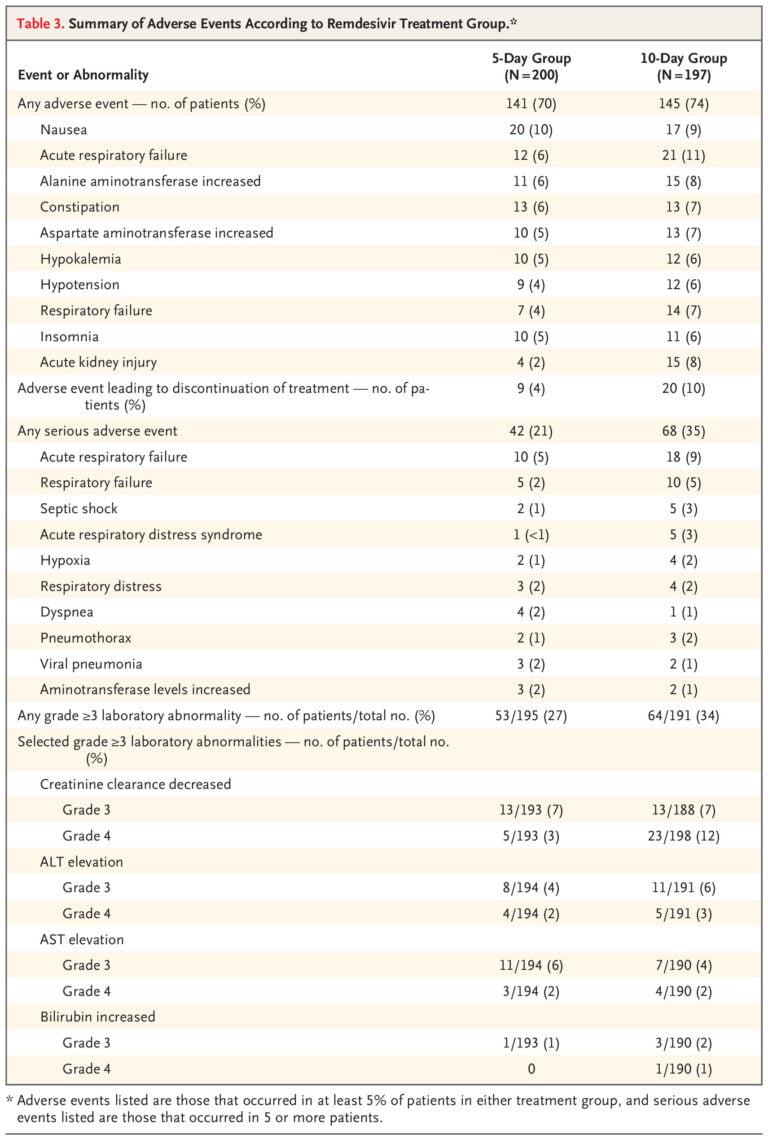
In a randomized, open-label clinical trial (Study GS-US-540-5773) of remdesivir in 397 subjects with severe COVID-19 treated with remdesivir for 5 (n=200) or 10 days (n=197), adverse events were reported in 71% and 74% of subjects, respectively, serious adverse events were reported in 21% and 35% of subjects, respectively, and Grade=3 adverse events were reported in 31% and 43% of subjects, respectively. Nine (5%) subjects in the 5-day group and 20 (10%) subjects in the 10-day group discontinued treatment due to an adverse event. All cause mortality at Day 28 was 10% vs 13% in the 5- and 10-day treatment groups, respectively.
Please do not miss the fact that there were reported 71% adverse events in the 5-day study and 74% adverse events in the 10-day study for patients taking remdesivir. 21% suffered serious adverse events in the 5 day study and 35% of the patients suffered serious adverse events in the 10-day study. Below is the chart of adverse events published in the study.
Hiding Remdesivir Adverse Events
Study GS-US-540-5773 was a randomized, open-label clinical trial in hospitalized adult subjects with severe COVID-19 treated with VEKLURY 200 mg on Day 1 and 100 mg once daily for 5 (n=200) or 10 days (n=197). Adverse reactions were reported in 33 (17%) subjects in the 5-day group and 40 (20%) subjects in the 10-day group. The most common adverse reactions occurring in at least 5% of subjects in either the VEKLURY 5-day or 10-day group, respectively, were nausea (5% vs 3%), AST increased (3% vs 6%), and ALT increased (2% vs 7%). Rates of any adverse reaction, serious adverse reactions, and adverse reactions leading to treatment discontinuation are presented in Table 6. [Chart 6 indicated that 3% of the 5 day group and 5% of the 10 day group had treatment discontinued due to adverse reactions.]
Notice the differences in reporting. The May 2020 report describes adverse events, whereas the October 2020 report changes the reporting to adverse reactions. The difference is that an adverse reaction denotes a causal relationship and an adverse event is an event that may or may not be causally related. A reaction is sometimes defined as the response to a medication where that response is at least reasonably possible to have been caused by the medication. By concealing the adverse events and only reporting adverse reactions, the October 2020 FDA report conceals the real danger from Veklury® (remdesivir). Keep in mind that an adverse reaction must be established by a reasonable possibility. Such nebulous standards for distinguishing adverse events from adverse reactions are ripe for abuse. An adverse event could be causally related but the reviewer may just decide it is not reasonable to infer it is causally linked, and thus it would not be called an adverse reaction.
May 2020 FDA Publication: “397 subjects with severe COVID-19 treated with remdesivir for 5 (n=200) or 10 days (n=197), adverse events were reported in 71% and 74% of subjects”
October 2020 FDA Publication: “Adverse reactions were reported in 33 (17%) subjects in the 5-day group and 40 (20%) subjects in the 10-day group.”
May 2020 FDA Publication: Nine (5%) subjects in the 5-day group and 20 (10%) subjects in the 10-day group discontinued treatment due to an adverse event.
October 2020 FDA Publication: 3% of the 5 day group and 5% of the 10 day group discontinued treatment due to an adverse reaction.
May 2020 FDA Publication: Serious adverse events were reported in 21% and 35% of subjects, [in the 5 day and 10 day groups] respectively.
October 2020 FDA Publication: Serious adverse reactions were reported in 2% and 2% of subjects in the 5 day and 10 groups respectively.
This is where the deception becomes obvious. The study did not measure aderse reactions! The study protocols for GS-US-540-5773 published by Gilead states that they were only going to measure adverse events. There is no mention of any plan to measure advers reactions.
Indeed, when one read the data from the Gilead study (GS-US-540-5773) itself there is only a recording of adverse events. There is no measure or memorialization of adverse reactions. So, the question is, if Gilead did not plan to measure adverse reactions and there is no record of such measures, where did the adverse reaction figures come from?
Majority of Patients on Remdesivir Suffer Liver Damage
Amazingly, in the May 2020 FDA publication indicated that a majority of the participants in the several remdesivir studies conducted have suffered liver damage.
Transaminase elevations have been observed in the remdesivir clinical development program, including in healthy volunteers and patients with COVID19. In healthy volunteers who received up to 150 mg daily for 14 days, alanine aminotransferase (ALT) elevations were observed in the majority of patients, including elevations to up to 10 times baseline values in one subject without evidence of clinical hepatitis.
The FDA report stated that in the GS-US-540-5773 study 5% of the patients suffered moderate to severe liver damage. Whereas, 2% of the study patients suffered severe liver damage.
Kidney Damage From Remdesivir is Foreseeable
Another foreseeable side effect of remdesivir is kidney damage. The FDA pubication reveals that “[i]ntravenous administration (slow bolus) of remdesivir to rats at dosage levels of =3 mg/kg/day for up to 4 weeks resulted in findings indicative of kidney injury and/or dysfunction.”
Invasive Mechanical Ventilation Required
In another later published study (ACTT-1, NCT04280705) reported in the October 10, 2010 FDA emergency use auhthorization that alleged to show the benefits of remdesivir, 27% of the patients taking remdesivir “were on invasive mechanical ventilation.” There was no control group in that study. It seems that the ventilation was the result of remdesivir because the study revealed that “[s]ubjects on mechanical ventilation at screening were excluded” from the study.
Early Study Termination Due to Adverse Events
In another human study conducted in China, 12% of the remdesivir group participants had to discontinue therapy with remdesivir due to adverse side effects. That compared to 5% in the control group.
Keep in mind that the control group in the Chinese’s study was not truly a placebo group and the remdesivir group was not truly a remdesivir group. Both the control group and the remdesivir group received corticosteroids, lopinavir/ritonavir, and interferon alfa-2b. The study was terminated early without any conclusions. The NIH admitted that “[t]he use of concomitant medications (corticosteroids, lopinavir/ritonavir, interferon) may have obscured the effects of remdesivir.”
Another human study cited did not have a control group, and the NIH, therefore, admitted that “it is not possible to assess whether the use of remdesivir led to the improvement.”
Remdesivir Proven Ineffective in Ebola Study
There was only one other human study cited, and the results were devastating for the patients in that study who were administered remdesivir. In that study, remdesivir was compared to three other treatments for Ebola. The control group was not actually a placebo group. The group was administered a medicine identified as ZMapp (a triple monoclonal antibody agent).
There was something strange about the trial. In another trial study 22% of the study patients died within 28 days using ZMapp on patients with Ebola. But in the comparative study with remdesivir the mortality rate for the control group using ZMapp shot up to 49.7% during the 28 day study.
The study administrators could only guess as to why their study patients were dropping like flies. They said: “The reason that mortality among patients who received ZMapp was 22% in the PREVAIL II trial (conducted during the outbreak in West Africa) and 50% in our trial (conducted during the current outbreak in the DRC) is unclear.”
One thing that was clear was that the significantly higher mortality for ZMapp brought the control group closer to the 53.1% mortality rate of the remdesivir group with the effect that remdesivir was shown to be merely less effective rather than extremely deleterious. That higher mortality of 49.7% for ZMapp also had the effect of showing that the other two treatment modalities were effective as compared to the control.
In any event, as the chart published in the study below reveals, remdesivir had the highest mortality of any of the treatment modalities with 53.1% of the Ebola patients who were administered remdesivir dying within 28 days.
Yet, with those studies showing the remdesivir is unsafe and ineffective, the NIH recommended remdesivir as the treatment for COVID-19. The results were foreseeable. Its use to treat patients with COVID-19 were predictably ineffective and unsafe. Please watch Dr. Ardis’ interview in the video below.
The NIH even now warns about renal failure and liver toxicity from Remdesivir. The World Health Organization (WHO) – does not recommend it for use in Covid patients. Fauci does.
Sources:
- https://jamesfetzer.org/2021/08/edward-hendrie-doctor-reveals-that-remdesivir-was-the-real-cause-for-many-alleged-covid-19-maladies/