
Lockdown
The coerced economic “shutdowns”—enforced with fines, arrests, and revoked business licenses—are not the natural outgrowth of a pandemic. They are the result of policy decisions taken by politicians who have suspended constitutional institutions and legal recognition of basic human rights. These politicians instead imposed a new form of central planning based on an unproven, theoretical set of ideas about police-enforced “social distancing.” Officials said an economic analysis of stay-at-home orders across the U.S. cost the economy $20 billion per day. Meanwhile, the CCP’s use of social media bots and other disinformation tactics promoted its own totalitarian response to the coronavirus pandemic and attacked its critics.
Suspending the rule of law and civil rights will have enormous consequences in terms of human life counted in suicides, drug overdoses, and other grave health problems resulting from unemployment, denial of “elective” medical care, and social isolation. None of that is being considered, however, since it is now fashionable to have governments determine whether or not people may open their businesses or leave their homes. So far, the strategy for dealing with the resulting economic collapse is no more sophisticated than record-breaking deficit spending, followed by debt monetization via money printing. In short, politicians, bureaucrats, and their supporters have insisted a single policy goal—ending the spread of a disease—be allowed to destroy all other values and considerations in society.
To some degree, the COVID pandemic has been portrayed as a morality play. Some would have you believe those who care about people support lockdowns; those who don’t care about people oppose them. We’re presented with false choices: we can support the economy or protect American lives. These types of arguments only serve to divide. They can also obscure a basic truth: there are human costs to lockdowns, besides the economic ones, that can ravage lives just as badly as any disease.
The same hypocrits in the media signalling these false virtues are the same leftist media and politicians who ignored lockdown rules for rioting and looting BLM and Antifa ‘peaceful protests’ but decried and shut down any actual protest regarding the tyrannous lockdown that was destroying businesses, forbidding worship services, or doing anything “normal” The “new normal is: riots = good, any other gathering = bad; abortion = good, church service (even in your car in a parking lot) = bad; funeral for a politically advantageous criminal victim = good; funeral for family member with more than 10 in attendance = bad, forbidden; Black Lives Matter, Looting in person = good, Voting in person = bad; Antifa = good, Police = bad. Welcome to the new normal.
Has it even worked? Mounting evidence says no.
Peru had one of the earliest (March 16th) and longest (four months) lockdowns. But it has the highest daily deaths per capita in the world now.
In The Lancet, Swedish infectious disease clinician (and World Health Organization (WHO) advisor) Johan Giesecke concluded:
It has become clear that a hard lockdown does not protect old and frail people living in care homes—a population the lockdown was designed to protect. Neither does it decrease mortality from COVID-19, which is evident when comparing the UK’s experience with that of other European countries.
At best, lockdowns push cases into the future, they do not lower total deaths. Gieseck continues:
Measures to flatten the curve might have an effect, but a lockdown only pushes the severe cases into the future—it will not prevent them. Admittedly, countries have managed to slow down spread so as not to overburden health-care systems, and, yes, effective drugs that save lives might soon be developed, but this pandemic is swift, and those drugs have to be developed, tested, and marketed quickly. Much hope is put in vaccines, but they will take time, and with the unclear protective immunological response to infection, it is not certain that vaccines will be very effective.
As a public policy measure, the lack of evidence that lockdowns work must be balanced with the fact that we have already observed that economic destruction is costly in terms of human life. Yet in the public debate, lockdown enthusiasts insist that any deviation from the lockdown will result in total deaths far exceeding those places where there are lockdowns. So far, there is no evidence of this.
In a new study titled “Full Lockdown Policies in Western Europe Countries Have No Evident Impacts on the COVID-19 Epidemic,” author Thomas Meunier writes, “total deaths numbers using pre-lockdown trends suggest that no lives were saved by this strategy, in comparison with pre-lockdown, less restrictive, social distancing policies.” That is, the “full lockdown policies of France, Italy, Spain and United Kingdom haven’t had the expected effects in the evolution of the COVID-19 epidemic.”1
The premise here is not that voluntary “social distancing” has no effect. Rather, the question is to whether “police-enforced home containment” works to limit the spread of disease. Meunier concludes it does not.
Meanwhile a study by polititical scientist Wilfred Reilly compared lockdown policies and COVID-19 fatalities among US states. Reilly writes:
The question the model set out to ask was whether lockdown states experience fewer Covid-19 cases and deaths than social-distancing states, adjusted for all of the above variables. The answer? No. The impact of state-response strategy on both my cases and deaths measures was utterly insignificant. The “p-value” for the variable representing strategy was 0.94 when it was regressed against the deaths metric, which means there is a 94 per cent chance that any relationship between the different measures and Covid-19 deaths was the result of pure random chance.
Overall, however, the fact that good-sized regions from Utah to Sweden to much of East Asia have avoided harsh lockdowns without being overrun by Covid-19 is notable.
Another study on lockdowns—again, we’re talking about forced business closures and stay-at-home orders here—is this study by researcher Lyman Stone at the American Enterprise Institute. Stone notes that areas where lockdowns were imposed either had already experienced a downward trend in deaths before the lockdown could have possibly shown effects or showed the same trend as the year prior. In other words, lockdown advocates have been taking credit for trends that had already been observed before lockdowns were forced on the population.
Stone writes:
Here’s the thing: there’s no evidence of lockdowns working. If strict lockdowns actually saved lives, I would be all for them, even if they had large economic costs. But the scientific and medical case for strict lockdowns is paper-thin.
Experience increasingly suggests that a more targeted approach is better for those who actually want to limit the spread of disease among the most vulnerable. The overwhelming majority—nearly 75 percent—of deaths from COVID-19 occur in patients over sixty-five years of age. Of those, approximately 90 percent have other underlying conditions. Thus, limiting the spread of COVID-19 is most critical among those who are already engaged with the healthcare system and are elderly. In the US and Europe, more than half of COVID-19 deaths are occuring in nursing homes and similar institutions.
This is why Matt Ridley at The Spectator quite reasonably observes that testing, not lockdowns, appears to be the key factor in limiting deaths from COVID-19. Those areas where testing is widespread have performed better:
Yet it is not obvious why testing would make a difference, especially to the death rate. Testing does not cure the disease. Germany’s strange achievement of a consistently low case fatality rate seems baffling—until you think through where most early cases were found: in hospitals. By doing a lot more testing, countries like Germany might have partly kept the virus from spreading within the healthcare system. Germany, Japan and Hong Kong had different and more effective protocols in place from day one to prevent the virus spreading within care homes and hospitals.
The horrible truth is that it now looks like in many of the early cases, the disease was probably caught in hospitals and doctors’ surgeries. That is where the virus kept returning, in the lungs of sick people, and that is where the next person often caught it, including plenty of healthcare workers. Many of these may not have realised they had it, or thought they had a mild cold. They then gave it to yet more elderly patients who were in hospital for other reasons, some of whom were sent back to care homes when the National Health Service made space on the wards for the expected wave of coronavirus patients.
We could contrast this with the policies of Governor Andrew Cuomo in New York, who mandated that nursing homes accept new residents without testing. This method nearly ensures that the disease will spread quickly among those who are most likely to die from it.
Meanwhile, Governor Cuomo saw fit to impose police-enforced lockdowns on the entire population of New York, ensuring economic ruin and ruined health for many non-COVID patients who were then cut off from vital treatments. Yet, disturbingly, lockdown fetishists like Cuomo are hailed as wise statesmen who “acted decisively” to prevent the spread of disease.
But this is the sort of regime we now live under. In the minds of many, it is better to abolish human rights and consign millions to destitution in the name of pursuing trendy unproven policies. The prolockdown party has even turned basic fundamentals of policy debate upside down. As Stone notes:
At this point, the question I usually get is, “What’s your evidence that lockdowns don’t work?”
It’s a strange question. Why should I have to prove that lockdownsdon’t work? The burden of proof is to show that they do work! If you’re going to essentially cancel the civil liberties of the entire population for a few weeks, you should probably have evidence that the strategy will work. And there, lockdown advocates fail miserably, because they simply don’t have evidence.
With economic output crashing worldwide and unemployment soaring to Great Depression levels, governments are already looking for a way out. Don’t expect to hear any mea culpas from politicians, but we can already see how governments are quickly moving toward a voluntary social-distancing, nonlockdown strategy. This comes even after politicians and disease “experts” have been insisting that lockdowns must be imposed indefinitely until there’s a vaccine.
The longer the lockdown-created economic destruction continues, the greater will be the threat of social unrest and even economic free fall. The political reality is thst the current situation cannot be sustained without threatening the regimes in power themselves. In an article for Foreign Policy titled “Sweden’s Coronavirus Strategy Will Soon Be the World’s,” authors Nils Karlson, Charlotta Stern, and Daniel B. Klein suggest that regimes will be forced to retreat to a Swedish model:
As the pain of national lockdowns grows intolerable and countries realize that managing—rather than defeating—the pandemic is the only realistic option, more and more of them will begin to open up. Smart social distancing to keep health-care systems from being overwhelmed, improved therapies for the afflicted, and better protections for at-risk groups can help reduce the human toll. But at the end of the day, increased—and ultimately, herd—immunity may be the only viable defense against the disease, so long as vulnerable groups are protected along the way. Whatever marks Sweden deserves for managing the pandemic, other nations are beginning to see that it is ahead of the curve.
Source: (Mises)
Other undiscussed consequences include a spike in violence, increased drug use and drug overdoses, increased child abuse cases, suicides (caused from depression of iolation, unemployment, more alcohol or drug use, etc.) As Antony Davies and James Harrigan wrote, “The uncomfortable truth is that no policy can save lives; it can only trade lives.” It may one day be determined that the lockdowns saved more lives than they destroyed, although recent evidence suggests the correlation between lockdown severity and COVID-19 deaths is weak. But let’s not underestimate the devastating human toll of this policy. The lives ruined or snuffed out by the lockdowns deserve better than that. They deserve to be seen.*
For those who understan the globalist agenda, the lockdown was never about ‘flattening the curve’. Bill Gates and the global elite want to eliminate a vast majority of the population to a controllable few hundred million, so they would be happy to see the curve as high as possible and the death rate at the initial guesstimate of 3.4% rather than the measly .002% it actually is/was. The lockdown was about destroying the booming economy (nearly 50 million Americans filed for unemployment during the lockdown) and exercising their political authority over the people to see if their fearmongering would lead us to give up a few more of our constitutional rights. Without declaring martial law, they got the vast majority of the world to play along – locked down at their homes, businesses forced to shut down as non-essential, locked out of their religious establishments, while abortion clinics were kept open as essential procedures, and many hospitals encouraged non-emergency, non-covid sick people (including many cancer patients) to stay at home. The Asch study says hi to all of the people bowing to the authoritative figures.
If the democrats can keep the lockdown going through the 2020 Election, or create a new fake pandemic in the fall for another lockdown, then they can justify the mail-in-ballot votes that they’ve been pushing. They can send in votes for all of the dead, all of the illegal immigrants, all of the prisoners they let out of jail, and maybe, just maybe …along with their other election fraud methods, steal this election from President Trump. If they could just get a little help from the media;)
An Illinois Judge voided Governor Pritzker’s coronavirus lockdown orders ruling: “Cannot Restrict Freedoms” Why can’t all judges be as wise?
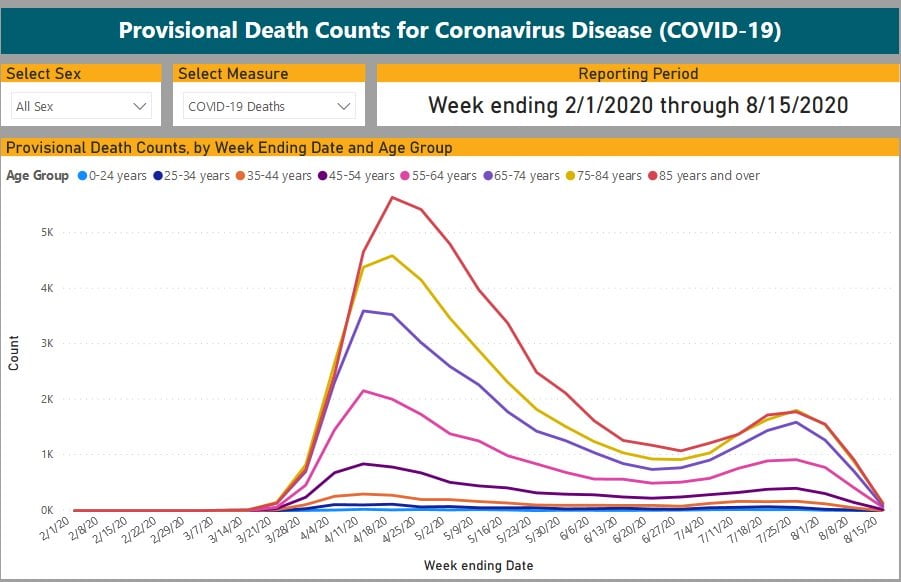
By mid-August deaths, even with the fraudulent ways of counting any death as a COVID-19 death, were essentially nil. Here’s a chart from the CDC:
Because of the decline, the controlled media shifted from even talking about deaths to exclusively talking ‘cases’ and every positive test, whether sick or not, was by then being counted as a ‘case’. The globalist agenda was to keep the scamdemic alive at least past the election so that mail-in voting could be deemed necessary.
As Joe Holt points out on the Gateway Pundit website:
What the data also clearly shows is that the number of deaths overall peaked back in April. The second wave (if you can even call it that) was not nearly as severe as the mortality numbers in April. The number of deaths continue to decrease overall.
A final observation is that for those under the age of 24 is almost non-existant. Based on this information, there is no reason to put in place any controls around our younger population. Masks or no masks, social distancing or not, those under the age of 24 are simply not dying from the China coronavirus.
A whistleblower from the University of Pittsburgh Medical Center, which operates a network of 35 hospitals in western Pennsylvania, described how the latest “surge” of Covid cases was overblown by the media. During this period, he said, hospitalizations increased from 96 beds to 600 beds, where the patients were kept in observation overnight and no deaths resulted. However, the media will report that there was a 600% increase in hospitalizations to make it seem more dire and to justify another lockdown. He claimed 90% or more of the covid beds were empty.
Here’s some of the tyranny, authoritarianism, hypocrisy and insanity we saw during the lockdowns:
- Disaster Declaration in All 50 States, Over 95% of U.S. Residents at Home
- Actor Kevin James Mocks Coronavirus Laws & “Karens” In Short Film
- California Sheriff Warns He Has the Power to Fine, Arrest People For Not Wearing Masks in Public
- Scotland’s top health official resigned after being caught traveling to her holiday home twice – in violation of her own stay-at-home demands for the rest of the country.
- Colorado Man Handcuffed in Front of His 6-Year-Old Daughter at Park For ‘Violating Social Distancing Order’ (VIDEO)
- Compilation- Authoritarianism Runs Rampant During Coronavirus Lockdown
- D.C. Mayor Shuts Down ‘Non-Essential’ Farmers and Fish Markets
- Democrat Kentucky Governor Announces Plan to Record License Plates of Easter Church Goers and Force Them to Self-Quarantine for 14 Days
- Didier Raoult- Government Study in Spain finds Those Who Kept Working Were Less Infected Than Those in Lockdown
- Dr. Fauci Says Americans Should Never Shake Hands Again Following His Highly Flawed Predictions on Coronavirus
- Facebook Working With State Governments to Take Down Coronavirus Lockdown Protest Announcements
- Gavin Newsom- Coronavirus Is ‘Opportunity for Reimagining a More Progressive Era’
- German Lawyer Who Criticized Lockdown Arrested, Taken to Psych Ward
- St. Louis Federal Reserve Head Says Americans Should Be Tested for COVID-19 Daily And Forced To Display a Badge on Their Clothing with the Result
- Google Not So Subtly Tracking Everyone During Covid-19 Panic
- Harvard Researchers Propose “Intermittent” Lockdowns – Through 2022!
- ID to Eat But Not to Vote- Washington Restaurants Ordered to Keep Log of All Customers, Including Contact Information
- Idaho Woman Facing 6 Months in Jail For Violating Coronavirus Lockdown Order by Holding Yard Sale
- Illinois Mayor Calls on Police to Crack Down on -Stay-at-Home- Violators – Then 48 Hours Later They Catch His Wife at a Bar
- In Late February, Nancy Pelosi Encouraged Large Groups to Congregate in Chinatown
- California Universities Cancel ‘In Person’ Classes for Fall Semester 2020
- Hong Kong’s 8 Million Continue Their Economic Shutdown Into the 4th Month – After 4 Coronavirus Deaths in 4 Months
- LA Mayor- “Snitches Get Rewards” & “Thank You For Turning Folks In”
- Mother Arrested, Her Screaming Child Ripped From Her Arms by Sydney Police For Violating Lockdown Order
- Michigan’s Crazed Governor Gretchen Whitmer Bans “Travel Between Residences”
- Mississippi Police Fine Christians $500 For Listening to Sermons While Parked in Their Cars (VIDEO)
- Mountain Biker Fined Over $1,000 for Driving to Exercise During Coronavirus Lockdown
- It’s Not About Your Health – What’s Really Going On with the Economic Lockdowns?
- Normal, Illinois Mayor Chris Koos Mocks Lock-Down Protesters and Laid Off Workers WHILE HE KEEPS HIS BIKE SHOP OPEN
- Police Hunt Down, Fine, Man Lying Alone on an Italian Beach
- Report- China Quietly Keeping Wuhan Residents Quarantined
- San Diego Police Issue Citations to People Parked in Their Cars Near the Beach For Violating ‘Social Distancing’ Order
- San Diego Police Ticket Dozens For Watching Sunset On Beach
- Scientist Whose Doomsday Models Sparked Global Lockdown Resigns After Breaking Quarantine To Bang Married Lover
- Seattle Cop Prepares To Be Fired After Refusing To Remove Viral Video Reminding Officers Not To Obey ‘Tyrannical Orders’
- Serbia Imposes 60-Hour ‘Total Ban on Movement’
- Spain- €2,000 Fine For “Disrespecting” a Police Officer During Lockdown
- Tampa Bay Pastor Arrested For Violating Social Distancing Orders Amid Coronavirus Pandemic
- Techno-Tyranny- How The US National Security State Is Using COVID-19 To Fulfill An Orwellian Vision – Zero Hedge
- Town Allows Cops to Fine Residents as Young as 12 for Violating “Stay-at-home” Order
- Tyrant- Democrat Governor Orders 14-Day Quarantine Of Easter Sunday Churchgoers
- UK Police Break Up ‘Prayer Meeting’ In Birmingham Park
- Undercover Cops Arrest Two Texas Women Offering Cosmetic Services From Home After Getting Tipped Off by a Snitch
- Video- Neighbor Gets Into Teen’s Face Because He’s Not “Social Distancing”
- Video- Police Drag Passenger Off Bus for Not Wearing Coronavirus Mask in Philadelphia
- Washington State Governor Inslee Warns Residents- Families with a Coronavirus Infected Member Will Not Be Allowed to Leave Their Homes
- Law Enforcement Tells Mississippi Pastor That His Rights Are Suspended, Worshippers Fined $500 for Attending Drive-In Service
- Welcome To Orwellian Italy 2020
- Wisconsin Supreme Court Strikes Down Governor’s Stay-at-Home Order
- US Navy orders draconian lockdown confining all sailors to barracks or bases. No church, no pools, no gyms, no restaurants, no sports, no movies! (Gateway Pundit Exclusive)
- PADDLEBOARDER BUSTED!!!Violates Stay-At-Home Order
- WWE Wrestling Deemed ‘Essential Business’ in Florida, Will Resume Filming Live Shows
- Bill de Blasio Responds to Massive ‘Black Trans Lives Matter’ Protest in Brooklyn by Welding Gates Shut at Biggest Park in Jewish Community where Kids were Playing
- WATCH: Orthodox Jews Cut Open Bill de Blasio’s Locked Parks
- Hairdressers ordered to be silent when salons reopen in two weeks to prevent virus spread
- Jack Dorsey’s Payment Processor Square Withholds 30% of Payments During Coronavirus Pandemic
- 76 Yr Old Scientist Arrested in Australia for for Skepticism of COVID-19 (VIDEO)
- Pregnant Aussie Mother Arrested for Allegedly ‘Inciting’ Coronavirus Lockdown Protest; Infowars report
- Gym Owners In San Fran Furious After Learning Government Gyms Have Been Open For Months
- Three Christians Arrested for Singing Church Hymns Outside in Idaho without Masks
- Young Mother TASED, CUFFED AND ARRESTED for Not Wearing Face-Mask at Mostly Empty Stadium to Watch HS Football Game
- Business Owners in Buffalo, New York Stand Up to Cuomo’s Covid Orders, Kick Out Sheriff and “Health Inspector” (VIDEO)
- 10 years in jail for stealing sweets? Thanks to Covid-19, it’s a possibility in Slovakia, and people are puzzled
- Adviser to Scottish Government Says People Should Wear Masks at Christmas Dinner
- Rules For Thee But Not For Me: Dr. Birx Caught Breaking Her Own COVID Guidelines
- Salon Owner Files Lawsuit Over Oregon Governor Threatening to Have CPS Take Her Kids for Defying Lockdown
- New Zealand Prime Minister Admits Using “Sustained Propaganda” To Spread COVID Fear
- California National Guard Put Fighter Jet on Alert For ‘Possible Domestic Mission’ to Terrify and Disperse Anti-Lockdown Protesters
- Duke University Hospital Denies Life Saving Kidney Transplant to Dying 14-Year-Old Girl for Being Unvaccinated
Social Distancing
There’s a reason that “social distancing” wasn’t a buzzword common to the American lexicon prior to 2020. There’s very little >science behind “social distancing” at all.
“It turns out,” Julie Kelly writes at American Greatness, “as I wrote last month, “social distancing” is untested pseudoscience particularly as it relates to halting the transmission of the SARS-CoV-2 virus. On its website, the CDC provides no links to any peer-reviewed social distancing studies that bolster its official guidance.”
There’s a reason for the lack of peer-reviewed studies on the CDC website. She continues:
The alarming reality is that social distancing never has been tested on a massive scale in the modern age; its current formula was conceived during George W. Bush’s administration and met with much-deserved skepticism.
“People could not believe that the strategy would be effective or even feasible,” one scientist told the New York Times last month. A high school science project—no, I am not joking—added more weight to the concept.
“Social distancing” is very much a newfangled experiment, not settled science. And, Kelley writes, the results are suggesting that our “Great Social Distancing Experiment of 2020” will be “near the top of the list” of “bad experiments gone horribly wrong.”
You also don’t have to be a scientist to also instinctively know that “two weeks to flatten the curve” becoming “America must lock down until a vaccine is created” is more social experimentation than science. But what the data have fleshed out, beyond the point of argument, is that the proximity of one human being to another has proven to be a very small factor in determining the impact of Covid-19 infections. What’s far more important is which human beings happen to be in close proximity of one another.
According to Dr. Steven Shapiro and the University of Pittsburgh Medical Center:
Crowded indoor conditions can be devastating in nursing homes, while on the USS Theodore Roosevelt 1,102 sailors were infected, but only 7 required hospitalization, with 1 death. This contrast has significant implications that we have not embraced. Epidemiologic prediction models have performed poorly, often neglecting critical variables.
The USS Theodore Roosevelt had a crew of 4,800. Given the acute sample, testing was holistic. This yields an actual infection rate of roughly 23 percent, and among those infected, the fatality rate is 0.09 percent. Among the Roosevelt’s entire crew of assumedly healthy and able-bodied sailors, on a floating Petri dish, during the thick of viral outbreak that shut down all schools and placed healthy citizens across America under house-arrest, the fatality rate was .002 percent.
It seems more than obvious that there is little sense in quarantining the young and healthy. As Dr. Shapiro also observes:
Our outcomes are similar to the state of Pennsylvania, where the median age of death from COVID-19 is 84 years old. The few younger patients who died all had significant preexisting conditions. Very few children were infected and none died. Minorities in our communities fared equally well as others, but we know that this is not the case nationally. In sum, this is a disease of the elderly, sick, and poor.
Here’s another thing you likely already know. Politicians and the media are committing to damage control to hide all of these facts from you. In fact, finding any news relating to Dr. Shapiro’s somewhat revelatory comments online is, so far, quite difficult.
That’s because, for the people who pushed “social distancing” and destroying the economy as an absolutely necessary evil, this is a matter of self-preservation. If this information were widely known, citizens might be more inclined to demand that schools and parks and restaurants and malls be opened. But if schools open tomorrow, without testing, and there is not a surge in hospitalizations or deaths, then the obvious question is why the schools closed in the first place. If restaurants and other shuttered businesses open without a spike in hospitalizations and deaths, then why did they ever close?
There’s value in the media and government officials maintaining the public perception that the costs of “social distancing” have been offset by its benefits. But while those benefits are elusive in the data, and require mountains of presumption to imagine that they even exist at all, the costs of “social distancing” couldn’t be clearer.
As Dr. Steven Shapiro concludes:
What we cannot do, is extended social isolation. Humans are social beings, and we are already seeing the adverse mental health consequences of loneliness, and that is before the much greater effects of economic devastation take hold on the human condition…
In this particular case, the problem we’re not going to be able to fix in the short term is the complete eradication of the virus. The problem we can fix is to serve and protect our seniors, especially those in nursing homes. If we do that, we can reopen society, and though infectious cases may rise as in the Theodore Roosevelt, the death rate will not, providing time for the development of treatments and
At this point, this is little more than common sense, and the truth can’t continue to be suppressed for much longer. It’s becoming more and more obvious that it’s well past time to take a more tactical approach to mitigation, as Dr. Katz suggested back on March 20, allocating resources and efforts toward protecting and caring for those most at-risk, and ending this soul-crushing and economy-crashing experiment with holistic “social distancing.”
Source: ZeroHedge
Even into mid-June and July, leftist politicians were clinging to social distancing. Writing for The Telegraph, Professors Carl Heneghan and Tom Jefferson, from the University of Oxford, said there is little evidence to support the restriction and called for an end to the “formalised rules”. The University of Dundee also said there was no indication that distancing at two metres (6 ft.) is safer than one metre.
Examining the current evidence for the two-metre rule, Prof Heneghan and Prof Jefferson looked at 172 studies cited in a recent review in The Lancet and found just five had dealt explicitly with coronavirus infection in relation to distance. Only one mentioned coming within six feet of a patient, and that paper showed proximity had no impact. Read full story here…
Face Mask Insanity
As shown by the research of Jon Rappaport whose been researching and reporting on the medical industry for over 30 years, and E.R. Nurse Patricia Neuenschwander pulling from research, experts, and professionals, there is absolutely no evidence to support that healthy people, especially children, wearing a mask is either safe or effective in any way. Yet, we are told by the media to be safe and wear them and required by some cities and states, like California (where Gov. Newsome oversteped his bounderies) and Ohio, and organizations, such as Costco, to wear them for entry into their stores. It has no basis and only induces fear, anxiety, and potential sickness for perfectly healthy people. Hmmm, just what the globalists want! How convenient.
(from NoMoreFakeNews) Mask wearers of the world, take them off—you have nothing to lose but your insanity…
Journal of the American Medical Association, April 17, 2020, “Masks and Coronavirus Disease”: “Unless you are sick, a health care worker, or caring for someone who has COVID-19, medical masks (including surgical face masks and N95s) are not recommended.”
At Children’s Health Defense, JB Handley has written an excellent article, “LOCKDOWN LUNACY: The Thinking Person’s Guide.” Here are two highlights from his section on masks:
“May 29, the World Health Organization announced that masks should only be worn by healthy people if they are taking care of someone infected with COVID-19:”
“’If you do not have any respiratory symptoms such as fever, cough or runny nose, you do not need to wear a mask,’ Dr. April Baller, a public health specialist for the WHO, says in a video on the world health body’s website posted in March. ‘Masks should only be used by healthcare workers, caretakers or by people who are sick with symptoms of fever and cough’.”
“…I often see this study from 2015 in the BMJ cited: ‘A cluster randomised trial of cloth masks compared with medical masks in healthcare workers’, and it bears repeating, since MOST of the masks I see people wearing in the community right now are cloth masks. Not only are these masks 100% ineffective at reducing the spread of COVID-19, but they can actually harm you. As the researchers explain:”
“’This study is the first RCT of cloth masks, and the results caution against the use of cloth masks. This is an important finding to inform occupational health and safety. Moisture retention, reuse of cloth masks and poor filtration may result in increased risk of infection…’”
Of course, I understand that when people are conspiracy whackos wearing their masks, they don’t respond well to facts, even when those facts come from the very organizations they believe in with religious fervor.
Here is something else from the Washington State Nurses Association: “Reprocessing masks using toxic chemicals is not a solution”:
“Nurses are reporting that respirators and face masks at WSNA repre-sented Providence facilities are being collected for reprocessing using ethylene oxide to decontaminate. The EPA has concluded that ethylene oxide is carcinogenic to humans and that exposure to ethylene oxide increases the risk of lymphoid cancer and, for females, breast cancer.”
“WSNA sent a cease and desist demand to Providence facilities where our members work, demanding an immediate halt to the reusing of any face masks, including N 95 and other respirators, that have been decontaminated by the ethylene oxide cleaning process. In addition, WSNA is preparing complaints to be filed with the Washington State Department of Occupational Safety and Health, highlighting this workplace hazard.”
“WSNA believes that the reuse of face masks or respirators cleaned with ethylene oxide violates the employer’s legal duty to ensure that nurses and other health care workers are afforded a safe and healthful working environment. While hospitals have long used ethylene oxide to clean certain surgical equipment, it should not be used to decontami-nate face masks or respirators, through which nurses and other health care workers must breathe for many hours at a time.”
“…The CDC warns that ethylene oxide is carcinogenic and teratogenic, and that ‘inhalation of ethylene oxide has been linked to neurologic dysfunction and may cause other harmful effects to the wearer’.”
“Prolonged exposure to ethylene oxide can hurt eyes and LUNGS, harm the brain and nervous system, and potentially cause lymphomas, leukemia, and breast cancer. This extremely hazardous toxic chemical poses a severe risk to human health.” [CAPS are mine.]
Is the use of toxic ethylene oxide to treat masks widespread? According to the Chicago Tribune, way back in March, Medline Industries was reprocessing 100,000 medical masks a day. They applied to the FDA for permission to use ethylene oxide. But wasn’t the horse already out of the barn? Weren’t they already using the chemical? I’ve queried Medline to find out whether the FDA has approved their application.
And finally, I have a lone report about a person from the region of Piedmont, Italy, who checked out his medical mask, which he’d received in the mail from the Department of Civil Protection. He discovered it contained zinc pyrithione.
If true, this is ominous. Consulting a simple safety data sheet on the chemical, from Cayman Chemical, I found a succinct statement: “Toxic if inhaled.”
But of course, medical masks must be worn. The lockdown authorities tell us so. They know. They must know because, well, they’re on television. Keep breathing through that mask. It’s “safe and effective.”
SOURCES:
- https://www.chicagotribune.com/news/environment/ct-trump-medline-masks-ethlyene-oxide-cancer-20200429-vyutifcyhvekljpn4rqxkpcl3i-story.html
- https://jamanetwork.com/journals/jama/fullarticle/2764955
- https://childrenshealthdefense.org/news/lockdown-lunacy-the-thinking-persons-guide/
- https://www.wsna.org/union/kadlec-medical-center/update/reprocessing-mask-using-toxic-chemicals-is-not-a-solution
- https://www.caymanchem.com/msdss/29154m.pdf
…More on the mask BS:
Patricia Neuenschwander, M.S.N., R.N., C.P.N.P.-P.C., an emergency room nurse with over two decades of experience, the science doesn’t support healthy people wearing masks. When Neuenschwander found out that her grandchild’s Montessori preschool was going to require even toddlers to wear masks, she did a deep dive into the research to better educate herself and her grandchild’s school about mask-wearing. The info below is an abbreviated verion of the FULL ARTICLE HERE
An important study using science to evaluate cloth mask use to prevent infection was conducted in March 2011. It is a large, prospective, randomized clinical trial; and the first randomized clinical trial ever conducted of cloth masks. The international team of researchers concluded:
This study is the first RCT of cloth masks, and the results caution against the use of cloth masks. This is an important finding to inform occupational health and safety. Moisture retention, reuse of cloth masks and poor filtration may result in increased risk of infection. Further research is needed to inform the widespread use of cloth masks globally. However, as a precautionary measure, cloth masks should not be recommended for HCWs, particularly in high-risk situations, and guidelines need to be updated.”
More recently, researchers from University of Illinois at Chicago School of Public Health reviewed the scientific literature. While not an exhaustive review of masks and respirators as source control and personal protection equipment (PPE), this review was made in an effort to locate and review the most relevant studies of laboratory and real-world performance to inform our recommendations. The review, which has 52 citations, concludes:
“We do not recommend requiring the general public who do not have symptoms of COVID-19-like illness to routinely wear cloth or surgical masks because… There is no scientific evidence they are effective in reducing the risk of SARS-CoV-2 transmission”
A 2020 study in Seoul, South Korea looked at the effectiveness of surgical and cotton masks in blocking COVID-19 in a controlled comparison of four patients. The COVID-infected patients were put in negative pressure isolated rooms. The scientists compared disposable surgical masks (3 layers) with reusable cotton masks.
Patients were instructed to cough 5 times while wearing no mask, surgical mask, or cotton mask. Interestingly, all swabs from the outer masks—including surgical masks—were positive for COVID-19. Inner masks were also found to be contaminated. That means the mask did not effectively filter out the COVID virus since it is too small. The authors assert:
Neither surgical nor cotton masks effectively filtered {COVID-19} during coughs by infected patients.” Conclusion: “both surgical and cotton masks seem to be ineffective in preventing the dissemination of SARS–CoV-2 from the coughs of patients with COVID-19 to the environment and external mask surface.”
“There is no specific evidence to suggest that the wearing of masks by the mass population has any potential benefit,” Dr. Mike Ryan, an epidemiologist who specializes in infectious diseases and public health and who is the executive director of the WHO health emergencies program, said at a media briefing. “In fact, there’s some evidence to suggest the opposite in the misuse of wearing a mask properly or fitting it properly” (source).
The CDC has known for decades that the influenza virus is transmitted person to person, but we have never been told to wear a mask to stop the spread of that virus. As a matter of fact, the CDC specifically says masks don’t work; and they do not recommend wearing a mask, to prevent transmission of the flu!
No recommendation can be made at this time for mask use in the community by asymptomatic persons, including those at high risk for complications, to prevent exposure to influenza viruses” (source).
Masks make children fearful
I have not been able to locate any published research on the psychological or emotional effects of having healthy children wear masks daily for hours at a time. I can only make an educated assumption based on over two decades of working as a healthcare professional that forcing children to wear masks will cause fear, anxiety, and negative feedback from caregivers. Mask wearing will affect children differently based on their developmental level. You cannot explain to a two-year-old why they are being forced to cover their nose and mouth.
Covering the mouth and nose for hours is not only uncomfortable for children (and adults), it also limits the airflow and the flow of oxygen coming in. It causes children, as with adults, to breath their own carbon dioxide, which we know is harmful. In addition, it provides a dark, warm, moist environment that potentially increases the risk of infection.
I’m just going to leave this here. 👇🏻 pic.twitter.com/NP4dH2GNbY
— MdKnightBabe™ (@MdKnightBabe) June 23, 2020
Fear is driving this recommendation for healthy people to wear masks, not science.
According to psychiatrist and medical legal expert Dr. Mark McDonald, the true public health crisis is not COVID-19 itself; rather, it’s the fear of the infection, which has “morphed and evolved into a form of mass delusional psychosis.” Many enter a state of hysteria when they see an unmasked person, even if they look perfectly healthy and clearly are not suffering from any kind of respiratory issue. This is a highly irrational state that has no basis in reality. Delusion is defined as believing something that doesn’t conform with reality.
There are serious concerns about the lasting effects this widespread insanity will have on children as they grow up. One of the worst traumas children suffer as a result of all this fearmongering is the idea that they may kill their parents or grandparents simply by being around them. Treating the children’s trauma in therapy is not going to be enough, as parents and other adults are the ones creating the trauma by their own exaggerated fear response. To heal a generation of traumatized children, we must first address the psychosis of the adult population.
As a nurse for over 25 years and holding a Master’s Degree in Science, I cannot in good conscience allow my grandchild to be subjected to an intervention that may cause physical, emotional, and psychological harm without being provided significant evidence that the benefits of such intervention outweigh the risks.
Should we be encouraging healthy people to wear masks? The answer is unequivocally no.
See also:
- Wearing masks may increase your risk of coronavirus infection, expert says
- Suffocation and Break Outs: Face Masks Wreaking Havok on the Human Body
- Registered Nurse Danika Bueno explains why wearing a face mask for long periods can be harmful to the body.
- Former neurosurgeon says masks are ineffective against COVID-19 and can cause health problems
- Neurosurgeon Says Face Masks Pose Serious Risk to Healthy and that There is No Scientific Evidence that it is Effective vs. COVID-19
- Dr. Fauci Admits Face Masks are Ineffective Against Coronavirus
- Texas Judge Says Mandatory Face Mask Requirement is Unconstitutional
- Kudos to Senator McClintock for refusing to abide by Chairman Nadler’s attempt to mandate masks in a house meeting
- London Mayor: Mandatory Masks Will Be The “New Normal” For At Least Another Year
We were tricked. Like this:
Continued on next page…